Player Classification
Classification an Overview
By Don Perriman IWBF Classification President
The classification of wheelchair basketball players has evolved significantly over the past 10 years. No longer is it necessary to individually examine each player in a medical room, debating about the relative grades of single muscles, and making subjective assessments of the balance attributes of a player before assigning them to a given class.
Players are now classified in their playing environment, on the basketball court, and in they're playing wheelchair. This enables the classifier to assess each player, as they will be when taking part in the actual competition.
Classification Philosophy:
Wheelchair basketball classification is based on the players' functional capacity to complete the skills necessary to play - pushing, pivoting, shooting, rebounding, dribbling, passing and catching. It is not an assessment of a player's level of skill, merely their functional capacity to complete the task. In particular, the trunk movement and stability observed during these actual basketball situations, forms the basis for the assignment of a player to a particular class.
Classes:
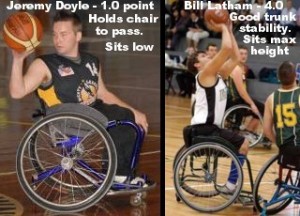
Players are assigned points as their classification - 1, 2, 3, and 4 are the recognized classes, with 0.5 classes between for the exceptional cases which do not fit exactly into one class, and the 4.5 category for the player with least or minimal disability.
Volume of Action:
Classes are defined according to players' "volume of action". Each class has a clearly defined maximal volume of action, which the player may exhibit. The volume of action refers to the extremes to which a player's trunk stability will allow them to reach, without holding on to the wheelchair, before overbalancing.
Class Characteristics:
Each class has characteristics unique to that class, which are used by the classifier. These characteristics are evident in each of the basketball skills observed as part of the classification process.
How to Classify:
Players are observed in their competition wheelchairs, complete with all strapping they will use, but in a training situation before the tournament commences. From this initial observation a player is assigned a class with which they will begin the tournament. The player is then observed in an actual competition game, at which time their classification will be confirmed or modified if the classification panel feels it is necessary. Only a new player who has not been previously Internationally classified need undergo this process. Players holding an International card do not require re-classification at each tournament they attend.
Team Balance:
The total number of points allowed on court at any time is 14.0. That is, the total points of all five players actually playing. If a coach allows the team to have over 14.0 points, they will incur a technical foul on the bench.
SCROLL DOWN FOR THE CLASSIFICATION TABLE
| Classification | |||||
| Function | Class 1 | Class 2 | Class 3 | Class 4 | Class 4.5 |
| Shooting | Significant loss of stability in the trunk as the shooting arm is extended over the head during follow through, often requiring arm support following the shot. During a two-handed shot, the trunk makes contact with the back of the wheelchair. Loses trunk stability during minimal contact. |
Mild to moderate loss of stability in the lower trunk during arm elevation and follow through, resulting in movement of the lower trunk away from the back of the wheelchair. Able to rotate the trunk toward the basket while shooting with both hands. |
Excellent stability of the trunk while sitting upright, particularly in follow-through of the shot. The trunk moves toward the basket with shooting movement, without loss of stability. |
Is able to move the trunk forcefully in the direction of the follow-through after shooting. Can lean laterally or rotate with a lateral lean to at least one side (away from the defender), while keeping both hands elevated and in contact with the ball. |
Is able to move the trunk forcefully in all directions during shooting, including lateral lean and lateral lean with rotation to both sides while keeping both hands in contact with the ball. |
| Passing | A forceful one-handed pass requires grasping with the off hand to maintain stability. The two-handed chest pass can only be executed with support of the back of the wheelchair or by resting on elevated knees. Unable to rotate to receive an over-the-shoulder pass without using one hand on wheelchair or leg to turn trunk. |
Little to moderate loss of trunk stability during one and two-handed passing, requiring holding the wheelchair or leg with the off hand. Fair stability when catching passes in an upright position. Is able to rotate the trunk to receive an over-the-shoulder pass with two hands using some support of the back of the wheelchair. |
One-handed and two-handed passes can be executed without using arm or back support to maintain stability. Can exert force in passing by trunk extension before initiating trunk flexion movement. Able to achieve near maximal rotation to catch over-the-shoulder passes with both hands without support of the back of the wheelchair. |
Able to flex, extend and rotate the trunk maximally while performing both one-handed and two-handed passes. Able to lean laterally to at least one side while executing a two-handed pass in the same lateral direction. |
Able to move the trunk in all directions with good stability while passing. Able to lean to either side while executing a two-handed pass in the same lateral direction. |
| Rebounding | Almost always reaches with one hand while holding the wheelchair to stabilize trunk with opposite hand. If a player uses two hands over the head, he will be in contact with the back of the wheelchair and easily lose stability during minimal contact. |
Usually rebounds with one hand, with minimal to moderate loss of stability. Two-handed over the head rebounds can be executed but are often accompanied by moderate loss of stability, especially during contact. |
Can rebound forcefully with two hands from overhead by moving the trunk forward while reaching for the ball. Limited stability during reaching laterally for rebounding; often executed by holding the side of the wheelchair with the off hand. |
Can lean forward and to at least one side to grasp an over-the-head rebound with both hands. | Can lean forward or to either side with arms overhead to grasp the ball. |
| Pushing the Wheelchair | In an upright position, the player leans into the back of the wheelchair, with head movement forward and back with each push. Some players rest the flexed trunk on elevated knees for support while pushing, away from the back of the wheelchair. |
Able to push the wheelchair without total support of the back of the wheelchair. Some loss of stability noted primarily at waist level with forward movement of the upper trunk accompanying each pushing motion, without movement of the lower trunk. |
Able to push the wheelchair forcefully with no loss of anterior or posterior stability. Upper and lower trunk move as a unit in exerting force during pushing movements. Pushing movement is usually with legs together. |
Able to push and stop the wheelchair with rapid acceleration and maximal forward movement of the trunk. Pushing movement is usually with legs apart. |
Same as Class 4 |
| Dribbling
|
Usually performed at the side on the wheelchair with trunk instability and slow acceleration. Some players may dribble in front of the footrests while resting the trunk on elevated knees for stability. |
Usually dribbles the ball beside the front castors, particularly when starting when this action is often accompanied by an initial loss of stability. Some players may dribble directly in front of the front castors especially when the trunk is supported by high placement of the knees. |
Can dribble the ball in front of the castors with one hand while simultaneously accelerating at a rapid rate by pushing forcefully with the other hand. The trunk flexes forcefully forward in the direction of the dribble. |
Can dribble the ball well in front of the front castors while pushing with the other hand. Can accomplish rapid speed and direction changes without loss of trunk stability during dribbling. |
Same as Class 4. |
| Optimal Wheelchair Positioning | Knees higher than hips. Knees strapped together or thighs and legs strapped to the wheelchair. Wheelchair back to mid-thoracic height, with upholstery slightly loosened to provide support for unstable trunk. May gain considerable stability by strapping upper trunk to wheelchair back. |
Knees higher than hips. Knees strapped together. Wheelchair back to waist level or slightly higher. May find it helpful to strap lower trunk to wheelchair back. |
Knees slightly higher than hips. Low wheelchair back, below waist level, allowing for full trunk rotation. |
May benefit from positioning of knees slightly higher than hips for maximal wheelchair mobility and speed. Alternatively, may position knees at same height as hips to achieve maximal height advantage. Low wheelchair back, allowing for full trunk rotation. Wearing leg braces or prostheses or strapping to the wheelchair seat may increase stability. |
Same as Class 4. |
| Typical Disability | T1-T7 paraplegia without abdominal muscle control Post-polio paralysis with arm involvement and without control of trunk musculature. |
T8-L1 paraplegia. Post-polio paralysis without control of lower extremity movement. |
L2-L4 paraplegia, with control of hip flexion and adduction movements, but without control of hip extension or abduction. Post-polio paralysis with minimal control of lower extremity movements. Hip disarticulation or above-knee amputees with very short residual limbs. |
L5-S1 paraplegia, with control of hip abduction and extension movements on at least one side. Post-polio paralysis with one leg involvement. Hemipelvectomy. Single above- knee amputees with short residual limbs. Most double above-knee amputees. Some double below-knee amputees. |
Single below-knee amputees. Some double below-knee amputees. Players with extensive orthopedic involvement of hips, knees or ankles. Post-polio paralysis with minimal (ankle/foot) involvement on one or both sides. |